Wednesday, 1:07am
Story In…
“You’re doing okay, the baby is out…one more little push. You have some bleeding, I’m going to press down a little here. Nurse, can you get me the Bakri balloon please. This is definitely a hemorrhage…” “Which Bakri do you want? The old or new model?” “I don’t know which is which, just get me one and assemble it please.” “Doctor, there is only the new model and I have never put this model together.” “Give it to me and call the the lab we need blood…shhh…why can’t I get this connected here…oops, the connector just fell. I need another balloon, I can’t use this connector because it fell on the floor.” “Doctor, each Bakri balloon is $500.00.” “I don’t care, I need another one, and get me the nurse manager, she is going to have to help us put this together…” “By the way, can someone check on where the blood is? It’s been 14 minutes already…she is bleeding out. I need another line in. Come on, ABCs remember, we are losing her…”
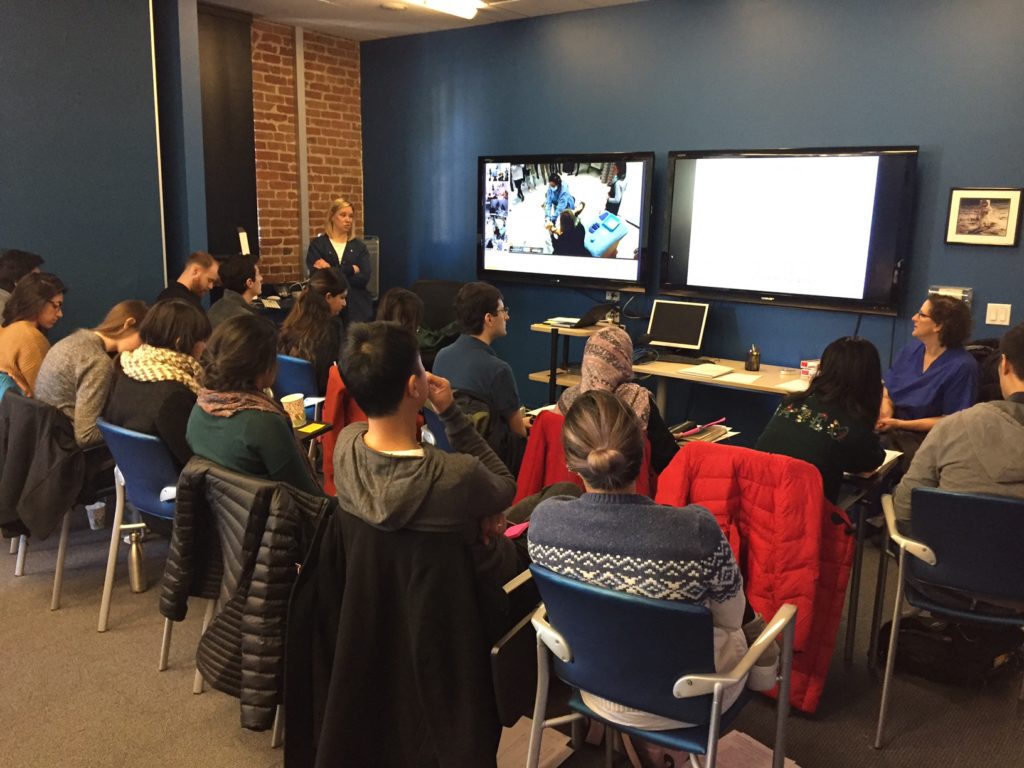
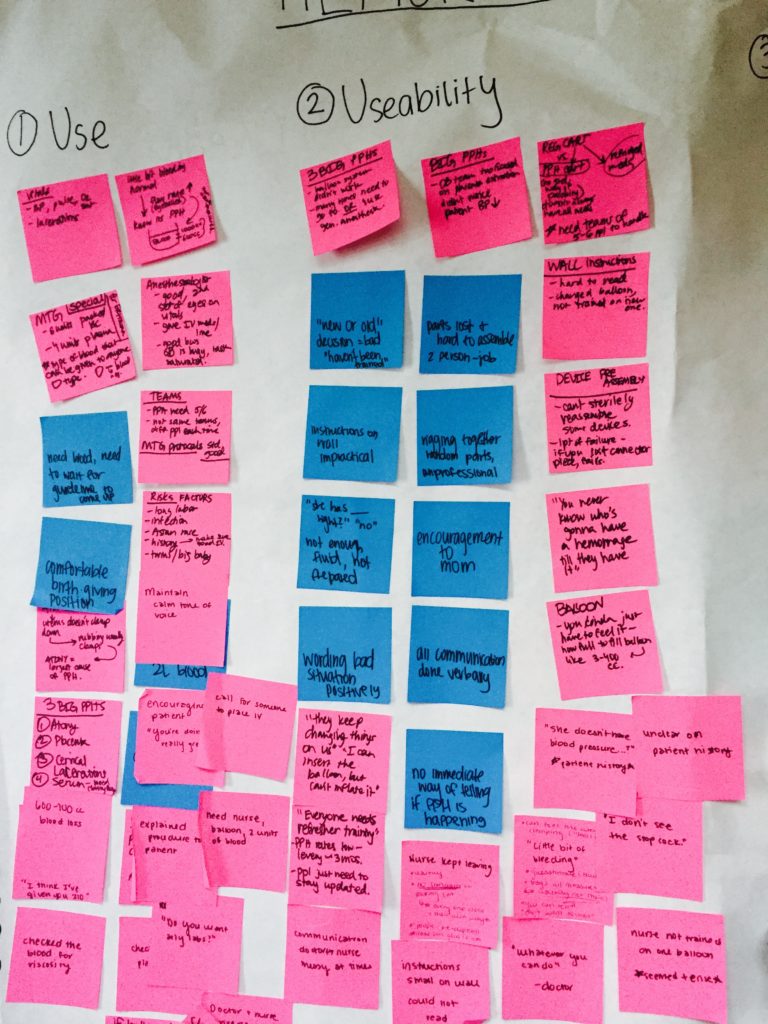
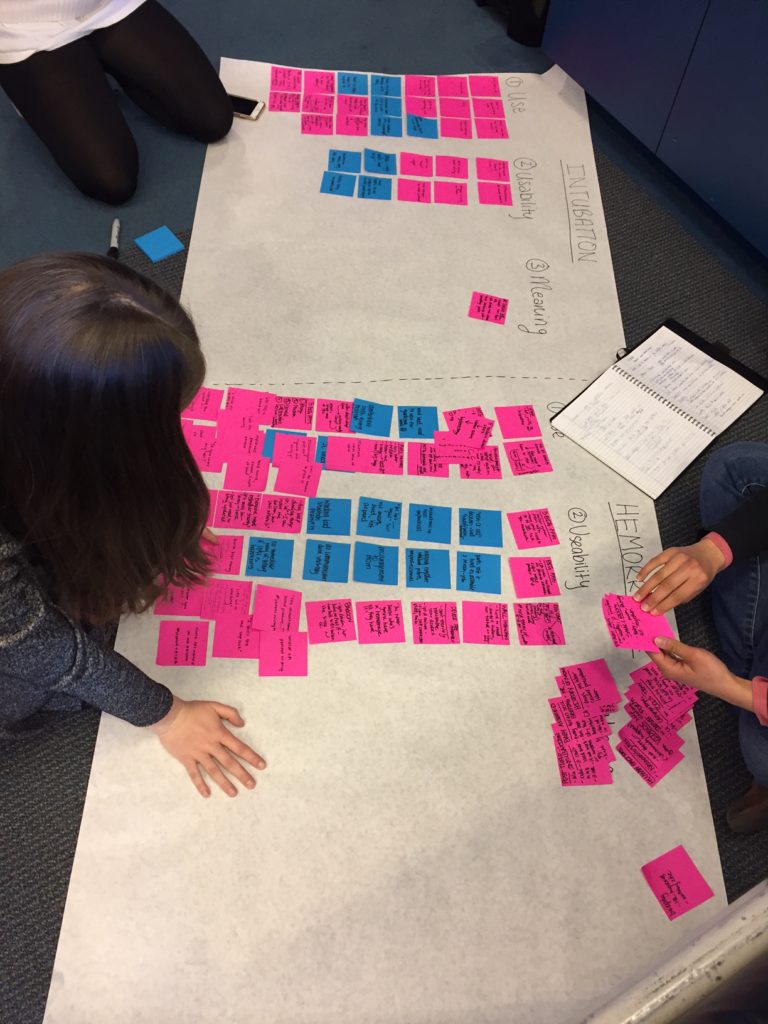
I recently co-taught a new workshop called Medical Device Design: Identifying Problems Through Observation. Our teaching team included myself, Nicole Yamada, MD, Neonatologist, Ruth Ann Crystal, MD, OB/GYN, and Julie Arafeh, RN, MSN. There were others that helped me put this workshop together. Notably Michael Barry, MS and Virginia Rath, PhD, MBA. This class included interdisciplinary graduate and undergraduate Stanford students. In this class I focused on teaching the first two phases of the design thinking paradigm, developing empathy and problem definition, using a complex medical environment as the backdrop. I talked about what kinds of techniques and tools designers use to develop empathy and synthesize information. Then, students observed a postpartum hemorrhage and an infant intubation simulation. We debriefed after the sims and interviewed the doctors. Students worked in small teams of two or three to synthesize their observations and interview take-aways. I asked the student to deliver the following for both observed procedures:
1) Bring a person/group to life and their healthcare situation to life. (Define the norm, or “story in”.)
2) Offer an insight “We were amazed to discover…”
3) An innovation is suggested “It would be game changing if…” (“story out”).
This workshop ran for three hours the first day and five hours the subsequent day, so we were quite limited in terms of time. I invited a panel of seven professionals to come and review the student presentations. They offered powerful feedback for the students and many of them stayed to chat after the presentations were over.

This workshop confirmed for me that the status quo tools used for intubation and maternal hemorrhage can certainly be improved, based on the challenges we viewed during the simulations as well as patient stories the clinical teaching team shared with us. Even after only a few hours of immersing themselves in the environment and with the users, our students came up with some astute insights and potential solutions. “Story Out” starts with: “It would be game-changing if…” Some examples of innovations were intubation tools that incorporated special sensors, a shared mental model data screen for OR healthcare workers and an improved design and packaging for the Bakri balloon.
Special thanks to Dr. Henry Lee, Dr. Louis Halamek and the d. School for supporting this workshop.
-Jules